This is the first of several articles I will be writing about Parkinson's disease (PD) and is a general introduction. I will go deeper into the different topics that I write about in this article in future articles.
PD is a progressive neurological disorder that affects millions of people worldwide, 4.4 cases per 100 000 people each year. This equates to over 200 Norwegians each year. The average age of those diagnosed with PD is about 60 years, but up to 10% of those diagnosed with PD are under the age of 50. According to the Norwegian Institute of Public Health, there were 18,000 people with PD in Norway in 2020, and this is expected to increase to 25,000 by 2040.
Parkinson's disease is characterized by the breakdown of specific parts of the brain that produce dopamine, the substantia nigra in the basal ganglia, which is essential for a number of brain functions. Including control of nerve signals to the muscles to control movement, and signals to parts of the brain that are important for good cognition. When the brain's ability to produce dopamine is reduced, both motor and non-motor symptoms can develop. These include stiff and slow movements, difficulty initiating movements, tremors, difficulty concentrating, and fatigue.
PD is a progressive disorder and the speed of its continuous deterioration varies between individuals. Early symptoms may be mild and go unnoticed, but as the disease progresses, symptoms become more severe and affect daily activities. The course of the disease can last for decades and there is currently no cure for PD. However, well-tailored rehabilitation has been shown to slow down the negative progression of symptoms.
The cause of PD is complex and multifactorial. Although there is no single cause of PD, it is believed that a combination of genetic and environmental factors contribute to the development of the disease.
Degradation of the basal ganglia
The basal ganglia are a group of nuclei in the brain that play an important role in the control of movement and cognition, among other things. In PD, degradation of the dopamine-producing neurons in the substantia nigra leads to a decrease in dopamine levels in the basal ganglia, disrupting the balance between activation and slowing in the circuitry. This results in an increase in the slowing down of nerve signals from the basal ganglia, leading to slow movements (bradykinesia), rigidity, and tremor, among other symptoms.
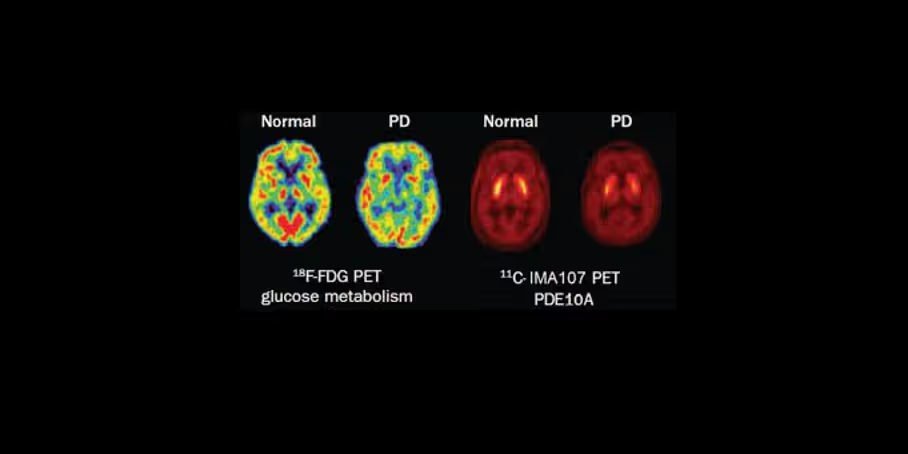
These images show the differences between a healthy brain and a brain with Parkinson's disease (PD). The images on the left show red areas illustrating activity. In the PD brain, you can see significantly less activity, especially in the center where the basal ganglia are located, but also in other areas that have less activity. It is also seen that the PD brain has increased activity in other areas compared to the healthy brain.
Secondary functional disorders of the brain
Degradation of the substantia nigra in the basal ganglia also leads to secondary brain dysfunctions that can contribute to exacerbation of symptoms and create new symptoms. Including impaired multisensory integration and impaired cross-modal communication causing both motor and non-motor symptoms. For example, impaired processing of visual impressions can lead to further problems with walking and balance, while impaired processing of sound can lead to problems with speech and concentration.
Multisensory integration is the ability of the brain to collect, align and process different sensory inputs, including the alignment and processing of different sensory inputs while doing an activity. You could say that it is the cooperation between our different senses.
Cross-modal communication is the brain's ability to share different sensory impressions and commands between different parts of the brain simultaneously. For example, centers in the brain responsible for visual impressions, movement information from joints and muscles, movement information from the balance organ in the inner ear, movement signals to muscles, and perception of touch and hearing need to interact and share information so that we can perform smooth and coordinated movements when getting dressed or eating. In simple terms, cross-modal communication in the brain can be described as a 'conversation' between the different parts of the brain that helps us to understand and interpret our environment in a more holistic way in order to perform intentional conscious and unconscious actions.
In order to function effortlessly in everyday life both physically and cognitively, our brain must be able to collect, process and coordinate different sensory impressions simultaneously. At the same time, the different parts of the brain are able to communicate with each other to plan an action, begin the execution of the action itself, and fine-tune it along the way to open the best possible outcome.
Motor symptoms
Motor symptoms in Parkinson's disease include tremors (tremor), slow movements (bradykinesia), stiff movements (rigidity) and impaired balance (postural instability). Tremor is the most common and recognizable symptom, and usually occurs in the hands, but can also affect any part of the body. Bradykinesia refers to slow movements, which can make it difficult to initiate and sustain activity. Rigidity refers to stiffness in the muscles, which can make movement uncomfortable and limit range of motion. Postural instability refers to difficulty maintaining balance, and can increase the risk of falls. The combination of these symptoms can make it very challenging to do normal everyday tasks such as grooming, cooking and eating.
Non-motorsymptoms
Non-motor symptoms in Parkinson's disease include difficulties with cognitive and executive challenges, and fatigue.
Impaired cognition includes impaired memory, attention and executive function. This can make it significantly more effortful to follow and concentrate on tasks at work, follow conversations and take in details during meetings, and difficulty planning and organizing tasks or events.
Fatigue is a common non-motor symptom of Parkinson's disease and can have a significant impact on quality of life. It is often described as an overwhelming feeling of exhaustion that is not relieved by rest. Fatigue can be caused by a combination of several factors, including sleep disturbances, depression and side effects of medication. However, neuroscience research also indicates that impaired multisensory integration and disrupted cross-modal communication cause the brain to overwork on simple tasks and may be a major contributor to fatigue.
Treatment
Although there is currently no cure for Parkinson's disease, there are a number of treatment options available to manage the symptoms of the disease. These include drug treatment, surgical procedures, and rehabilitation. The treatment methods used often depend on the severity of the symptoms, how the individual responds to the initial or ongoing treatment, and the progression of the disease. Regardless of which drug or surgical treatment is used, it has been shown that properly tailored rehabilitation can improve symptoms and slow the negative progression of symptoms in people with Parkinson's disease. Both the motor and non-motor symptoms.
Stay tuned for upcoming posts on Parkinson's disease. As I will go deeper into what happens in the brain in Parkinson's disease and how tailored rehabilitation can help improve symptoms.
Brain Camp has long and wide experience in the examination and customization of neurological rehabilitation for people with Parkinson's disease. Read about our about our approach or more about our rehabilitation stay.
Reference list:
1. Barbe MT, Tonder L, Krack P. Deep brain stimulation for movement disorders: a promising tool for unraveling the mysteryof the basal ganglia. Front Integr Neurosci. 2014; 8:73.
2. Baumann CR, Held U, Valko PO. Movement disorders andsleep-wake disturbances: a systematic review. J Neurol. 2020;267(5):1369-1386.doi:10.1007/s00415-019-09634-y
3. Cerasa A, Morelli M, Augimeri A, et al. Compensatorymechanisms in Parkinson's disease: A systematic review and meta-analysis. Neurosci Biobehav Rev. 2020;108:496-505.doi:10.1016/j.neubiorev.2019.11.014
4. Dalaker TO, Zivadinov R, Beyer MK. Brain structuralalterations in Parkinson's disease with mild cognitive impairment and dementia:a systematic review. J Neurol. 2021;268(1):1-11.doi:10.1007/s00415-020-10147-4
5. De Pablo-Fernandez, E., Lees, A. J., & Holton, J. L. (2021). Parkinson's disease pathology: from the cell to the clinic. Journal of Neurology, Neurosurgery &Psychiatry, 92(2), 201-213.
6. Deuschl, G., & Schade-Brittinger, C. (2020). Parkinson's disease:diagnosis and differential diagnosis. DeutschesÄrzteblatt International, 117(50), 844.
7. Espay, A.J., Lang,A.E. & Parkinson's Disease Foundation P4 Group (2020). Commonmisconceptions about Parkinson's disease. Lancet Neurology, 19(4), 290-299.doi: 10.1016/S1474-4422(19)30396-8
8. Fabbri, M., Guedes, L.C., Coelho, M., et al. (2020). Cognitive andneuropsychiatric features of Parkinson's disease. Expert Review of Neurotherapeutics, 20(8),835-853. doi: 10.1080/14737175.2020.1806904
9. FasanoA, Canning CG, Hausdorff JM, et al. Falls in Parkinson's disease: a complex andevolving picture. MovDisord. 2017;32(11):1524-1536.
10.Gao Y, Wang Y, Guo Y, etal. Theclinical features and mechanisms of Parkinson's disease: a review of recentresearch. Biomed Pharmacother. 2021;133:110972.doi:10.1016/j.biopha.2020.110972
11.Goldman JG, Litvan I. Mild cognitiveimpairment in Parkinson's disease. Minerva Med. 2011;102(6):441-459.
13.Huang, Y., &Halliday, G. M. (2020). Progress and perspectives on genetic research inParkinson's disease. Neural Regeneration Research,15(6), 1006.
14.Jankovic J, Poewe W. Therapies in Parkinson'sdisease. Curr Opin Neurol. 2012;25(4):433-447.
15.Kalia, L. V., &Lang, A. E. (2015). Parkinson's disease. The Lancet, 386(9996), 896-912.
16.Karakis I, MontenegroJD, Peña-Gómez C, et al. Multisensory Integration and Parkinson's Disease: ASystematic Review of the Evidence. ArchClin Neuropsychol. 2020;35(1):1-16. doi:10.1093/arclin/acz040
17.Kim SH, Kim J, Lee YJ,et al. Fatiguein Parkinson's disease: A systematic review and meta-analysis. Mov Disord. 2020;35(8):1386-1395. doi:10.1002/mds.28119
18.Kluger BM, Fox S, Timmons S, et al. The Characterization of Fatigue inParkinson's Disease. Parkinson's Dis. 2016; 2016:4592480.
19.Kordower JH, OlanowCW, Dodiya HB, et al. Disease duration and the integrity of the nigrostriatal system in Parkinson's disease. Brain.2021;144(2):596-612. doi:10.1093/brain/awaa430
20.Lee J, Kim J, Kim Y,Kim H, Jeon B. Clinical phenotype and progression of Parkinson's disease inKorean population-based cohort. Parkinsonism Relat Disord. 2020;79:58-63.doi:10.1016/j.parkreldis.2020.07.031
21.Liu H, Zhang X, Yan J,et al. Impairedsensory integration affects balance control and postural stability in patientswith Parkinson's disease: A systematic review and meta-analysis. Front Neurol.2020;11:542858. doi:10.3389/fneur.2020.542858
22.Lorrain D, Tang-WaiDF, McDonald C, Lang AE. Cognitive impairment in Parkinson's disease: a reviewof recent studies. Curr Opin Neurol.2021;34(4):514-519. doi:10.1097/WCO.0000000000000927
23.Obeso, J.A., Rodriguez-Oroz, M.C., Stamelou,M., et al. (2020).The expanding universe of disorders of the basal ganglia. Lancet Neurology, 19(5), 399-408. doi:10.1016/S1474-4422(20)30040-9
24.Poewe, W., Seppi, K.,Tanner, C.M., et al. (2020). Parkinson disease. Nature Reviews DiseasePrimers, 6(1), 65. doi: 10.1038/s41572-020-0209-3
25.Steffen, T., Seney,M.L., Neligan, A., et al. (2020). Multisensory integration in Parkinson'sdisease: a systematic review and meta-analysis. Movement Disorders, 35(11), 1941-1951. doi:10.1002/mds.28273
26.Thanvi BR, Lo TC. Long-term motorcomplications of levodopa: clinical features, mechanisms, and managementstrategies. Postgrad Med J. 2007;83(980):305-312.
27.Marsili, L., Rizzo,G., Colosimo, C., & Calandra-Buonaura, G. (2021). Non-motor symptoms inParkinson's disease: prevalence, pathophysiology and management. Expert Review of Neurotherapeutics, 21(2),131-145.
28.Munhoz, R.P., Espay,A.J., Morgante, F., et al. (2022). Therapeutic advances in Parkinson's disease. Movement Disorders, 37(1), 25-44. doi:10.1002/mds.28454
29.Norwegian Instituteof Public Health (2020). Parkinson's disease (in Norwegian). AccessedSeptember 24, 2021. https://www.fhi.no/nettpub/hin/psykisk-helse/parkinsons-sykdom/
30.Obeso JA, Rodriguez-Oroz MC, Goetz CG, MarinC, Kordower JH, Rodriguez M. Missing pieces in the Parkinson's disease puzzle.Nat Med. 2020;26(3):353-361. doi:10.1038/s41591-020-0788-8
31.Obeso, J. A., Rodriguez-Oroz, M. C., Goetz,C. G., Marin, C., Kordower, J. H., Rodriguez, M., ... & DeLong, M. R.(2010). Missing pieces in the Parkinson's disease puzzle. Nature Medicine, 16(6), 653-661.
32.Ponsen, M.M., Stam,C.J., Bosboom, J.L.W., et al. (2021). Brain network topology and the development ofcognitive and motor symptoms in Parkinson's disease. Parkinsonism & Related Disorders, 83,111-116. doi: 10.1016/j.parkreldis.2021.06.027
33.Postuma, R. B., Berg,D., Stern, M., Poewe, W., Olanow, C. W., Oertel, W., ... & MDS clinicaldiagnostic criteria for Parkinson's disease. Movement Disorders, 30(12), 1591-1601.
34.Sharma, S., Moon, C.S., Khundrakpam, B.S., etal. (2021).Alterations in white matter network topology in Parkinson's disease with mildcognitive impairment. Journal of Neurology, 268(6),1986-1996. doi: 10.1007/s00415-020-10153-9
35.Surmeier, D. J.,Obeso, J. A., & Halliday, G. M. (2017). Parkinson's disease is not simply aprion disorder. Journal of Neuroscience, 37(41),9799-9807.
36.Tysnes, O.B. & Storstein, A. (2017). Epidemiology ofParkinson's disease. Journal of Neural Transmission, 124(8), 901-905. doi:10.1007/s00702-017-1686-y
37.Van Rooden SM, Heiser WJ, Kok JN, et al. The basal ganglia: Focused selection andinhibition of competing motor programs. Prog Neurobiol. 2010;90(3):354-371
38.Videnovic A. Management of sleep disordersin Parkinson's disease. Mov Disord. 2017;32(5):659-668.
39.Zis, P., &Martinez-Martin, P. (2021). Non-motor symptoms of Parkinson's disease. Journal of Neural Transmission, 128(5),547-550.
40.Zuurmond, L.,Heimans, J.J., Skogseid, I.M., et al. (2020). Multidisciplinary care for patients with Parkinson's disease. LancetNeurology, 19(1), 66-68. doi: 10.1016/S1474-4422(19)30402-0