Positional dizziness -Benign positional paroxysmal vertigo (BPPV): Harmless, but inhibits quality of life.
.avif)
Positional dizziness means that dizziness is triggered when you change the position of your head, and can have various causes. Including neck tension and the brain's impaired awareness of neck movements, inflammation of the balance nerve, and the most common cause which is benign positional paroxysmal vertigo (BPPV). In Norway, also known as krystallsyken. In this article we will focus on BPPV, but we will write more about other forms of positional vertigo in later articles.
As mentioned, BPPV is the most common cause of dizziness, and research indicates that approximately 10% of the population will contract BPPV at some point in their lives. In Norway alone, more than 80,000 people are diagnosed with BPPV every year. The dizziness that accompanies BPPV can be very frightening and give an extremely intense sensation of rotatory dizziness, but it is not dangerous. Although BPPV is not a dangerous or life-threatening condition, it does not mean that it can inhibit or destroy quality of life. It must therefore be taken seriously, and investigated and treated by a competent healthcare professional.
Dizziness is a very common symptom, and as many as 20% of us suffer from some form of dizziness at times. Dizziness can be a secondary symptom as a result of a neurological disease or injury, or caused by an injury or disease of the balance organ in the inner ear or the balance nerve. Fortunately, in the vast majority of cases there is no life-threatening cause and there is usually always something that can be done to reduce the dizziness. Nevertheless, it is important to be examined thoroughly as soon as possible so that the right treatment can be initiated or referral to the right body can be made. If you experience other symptoms along with the dizziness. Including headaches, double vision, language difficulties or difficulty moving your arms or legs, it is very important to contact your doctor or emergency room to rule out serious conditions such as stroke.
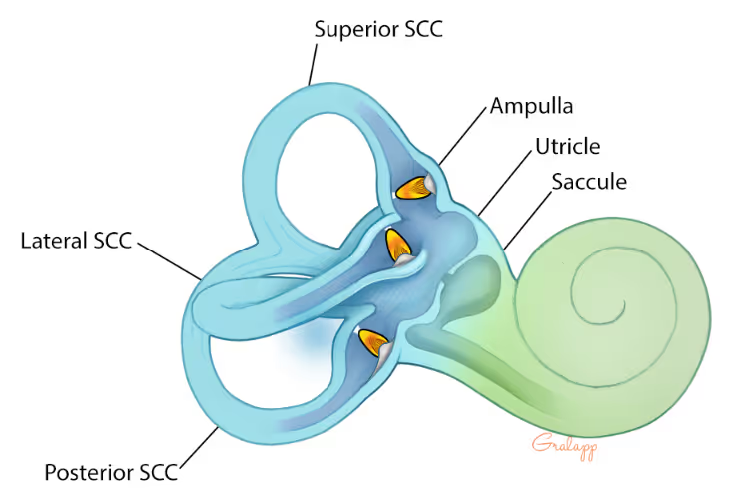
BPPV is a positional dizziness where particles (otoliths) become dislodged inside the balance organ (utriculus/sacculus) in the inner ear. This means that you experience dizziness when you change the position of your head, such as when you bend forward to put on shoes, turn around in bed, or stand up from lying to sitting. The particles stray into one or more archways, semi-circular canals, which are also part of the balance organ in the inner ear. These particles cause overactivation of sensory structures (cupula) in the archways that send movement signals to the brain, giving a false sense of movement. The brain is simply tricked into thinking you are in more motion than you are. At the same time as the brain experiences false movement, the balance organ sends too many signals to the muscles that move the eyes. This results in uncontrolled eye movements, which we call nystagmus. Each archway sends signals to specific eye muscles and causes characteristic eye movements that tell us which archway has loose particles and is the cause of BPPV. One of the most common tests to diagnose BPPV is the Dix-hallpike test. This test is performed by placing the head in a position so that particles that have strayed into the archways trigger positional vertigo and positional nystagmus.
This video demonstrates the positional nystagmus characteristic of BPPV in the left posterior archway.
There are two forms of BPPV: canalolithiasis, which is the most common type (approx. 80%), where the particles float freely in one or more archways. The other form of BPPV is cupulolithiasis, where the particles stick to the cupula itself.
BPPV can cause extremely intense dizziness that can be very disabling. However, BPPV is usually the easiest dizziness to treat if you have diagnosed the correct archway involved. Research shows that 70-90% of people with the most common type of BPPV in the posterior arch, canalolithiasis. Become completely free of dizziness after 1-3 treatments with repositioning maneuvers. These are exercises that make the particles float in place. But unfortunately, as many as 50% relapse within a few months or years.
Research also shows that even without treatment, about 70% will be free of dizziness within 4 weeks. However, as many as 30% of those with untreated BPPV are plagued with dizziness for 3 months or longer. Even if the dizziness resolves after 4 weeks without treatment, the patient is left with unnecessary discomfort and reduced quality of life for longer than those who receive treatment. And if you suffer from dizziness caused by BPPV for more than 3 months, chronic BPPV, there is a greater risk of developing other forms of dizziness syndrome that are significantly more complex to treat than BPPV. Including persistent postural perceptual dizziness (PPPD). We will write more about PPPD and other dizziness syndromes in a later article.
In most cases of BPPV, the cause is unknown, but you are significantly more likely to get BPPV if you have a metabolic problem, are in menopause, have diabetes, high cholesterol, migraine, have suffered head trauma such as a traffic accident or fall, and are over 50 years of age. Research shows that treating patients with BPPV can be more complicated and take longer if you are in one of these risk groups. Treatment of BPPV often needs to be combined with other rehabilitation, including vestibular rehabilitation therapy.
Treatment of dizziness and BPPV
Brain Camp has extensive experience of treating and rehabilitating patients with various forms of dizziness. After a short phone call, we decide what type of examination is recommended. If a cause other than BPPV is suspected, we recommend a comprehensive neurological examination lasting about 5 hours to identify which parts of the balance and sensory system need rehabilitation and how this rehabilitation should be best tailored. This examination includes video nystagmography, which analyzes purposeful eye movements to see how different parts of the brain and nervous system work, computer-based balance measurement, and tests that challenge different parts of the coordination system. The patient is also tested for BPPV, as it is possible to have causes of dizziness such as post-commotio syndrome, PPPD or Mal de Debarquement syndrome in combination with BPPV.
For patients where BPPV is suspected to be the cause of dizziness, we recommend a more targeted examination for BPPV lasting approximately 60 minutes. This examination includes a neurological examination to rule out serious disease, Dix-Hallpike test with video-oculography which is the standard test for BPPV, and tests for other types of postural dizziness. Video-oculography is an examination with a mask that has an infrared camera attached to analyze eye twitching, nystagmus, caused by BPPV. Video-oculography is important to better analyze the direction in which the nystagmus moves and how long the nystagmus lasts. This information tells us which archway has BPPV and what type of BPPV the patient has. This is essential, as the different archways and forms of BPPV require different treatment. For patients with BPPV, we are one of the few clinics in Europe that can offer examination and treatment in the TRV Chair in addition to providing thorough training on how to do the repositioning maneuver yourself as a home treatment.
TRV chairs developed by Dr. Thomas Richard-Vitton (TRV), a French ear, nose, throat specialist. The TRV chair is designed to rotate the patient 360 degrees in multiple planes, creating acceleration of the fluid in the archways to "shake" the particles loose in a more effective way than traditional maneuvers. Research shows that the treatment of BPPV in a TRV chair can be significantly more effective, and more gentle for patients who find it difficult to carry out the more traditional treatment methods due to, for example, neck injuries. Treatment using a TRV chair has been shown to be significantly more effective for those who suffer from chronic BPPV and frequent relapses, and for those who have BPPV in multiple archways. It also shows that treatment using a TRV chair can reduce the risk of recurrence or reduce the frequency of recurrence.
References:
- American Hearing research foundation.
- Abdul Kader Afif Yamout, 2022. Comparison of the effectiveness of TRV chair and canalith repositioning procedure (VRP) for the treatment of benign positional paroxysmal positional vertigo (BPPV). International journal of otolaryngology and head & neck surgery, 2022, 11, 143-153.
- Balanselaboratoriet.no
- Berit Hackenberg et al, 2023. Vertigo and its burden of disease-Results from a population-based study. Laryngoscope Investigative Otolaryngology. 2023.
- Bhattacharyya N, et al. 2008. Clinical practice guideline: benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 2008.
- Dimitris G, et al. 2011. Diagnosis of single- or Multiple-Canal benign paroxysmal positional vertigo according to the type of nystagmus. International Journal of Otolaryngology, vol 2011, page 13, 2011.
- Giuseppe Chiarella, wt al, 2017. Hashimoto thyroiditis and vestibular dysfunction. Endocrine practice 2017; 23: 7: 863-868.
- Gordon CR, et al. 2004. Is posttraumatic benign paroxysmal positional vertigo different from the idiopathic form?. Arch Neurol. 2004.
- Gordon CR, et al. 2005. Benign paroxysmal positional vertigo: who can diagnose it, how should it be treated and where? Harefua. 2005.
- Hansen S, Kalberg M. Benign ataropksysmal positional vertigo- the most frequent form of otogenic vertigo. Ugeskr Læger 2007; 169: 1996-2002.
- Crystal Sickness.com